Thyroid Issues? These are the Ten Labs You Need to Run.
Are you suffering from symptoms of thyroid dysfunction? Do you feel like your doctors are missing something? Do you feel terrible despite “normal” labwork?
Keep reading to learn which ten lab markers are critical to get to the bottom of your thyroid issues!
Hashimoto’s Disease
Autoimmune disease affects more people in the United States than cancer and heart disease. In fact, according to the National Institutes of Health 8% of the American population – 24 million people – have been diagnosed with an autoimmune disease, and the prevalence is on the rise.
But this is only the number of people diagnosed with an autoimmune disease. Researchers estimate there are close to 72 million people suffering from an autoimmune disease in the United States – 22% of our population.
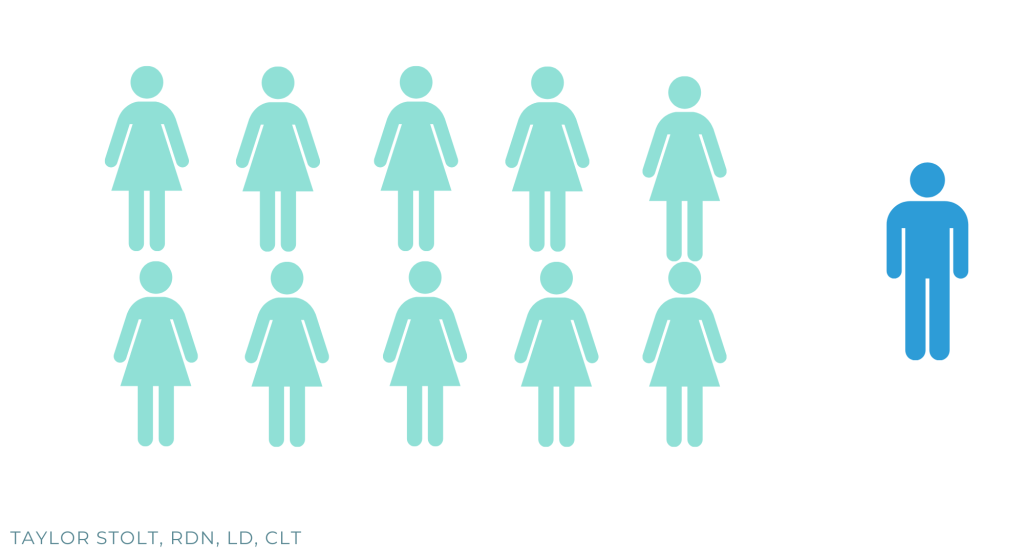
Thyroid autoimmune diseases are the most common autoimmune disease, affecting 7-8% of the US population. It is much more prevalent in women – the female to male ratio is greater than 10:1.
Were you diagnosed with hypothyroidism? You probably have Hashimoto’s! Hashimoto’s is the most common thyroid autoimmune disease and it is the leading cause of hypothyroid (low thyroid) function, accounting for over 90% of low thyroid cases.
Having unexplainable health issues? Read through the common Hashimoto’s symptoms below to see if your thyroid may be to blame. As the body attacks the thyroid, you can experience both hypo- (low) and hyper- (high) thyroid symptoms.
Common hypothyroid Hashimoto’s symptoms
- Fatigue
- Weight gain despite diet and/or exercise
- Morning headaches
- Depression
- Difficulty swallowing
- Brain fog/difficulty concentrating
- Constipation
- Cold hands and feet
- Numbness in hands and feet
- Muscle cramping
- Joint/muscle pain
- Needing excessive sleep to function properly
- Chronic digestive problems
- Itchy, dry skin
- Dry/brittle hair
- Hair loss (scalp and/or eyebrows)
- Heavy and/or irregular periods
- Facial swelling
- Difficulty conceiving
Common hyperthyroid Hashimoto’s symptoms
- Heart palpitations
- Inwards trembling
- Increased pulse
- Nervousness
- Anxiety
- Insomnia
- Night sweats
- Difficulty gaining weight
Wait a second – weight gain and weight loss can be signs of Hashimoto’s? Insomnia and fatigue?
I know, confusing.
This is where labwork is extremely helpful.
If you have a family history of thyroid issues, or you can relate to any of the symptoms above, labwork is a great next step to determine if your thyroid is functioning like it should be.
If you have already been diagnosed with Hashimoto’s but your doctor has only been checking your TSH level, keep reading to see what other labs are critical in order to get a complete picture of what is happening to your thyroid.

Is TSH enough?
If you talk to your doctor about checking your thyroid, most doctors will run only a TSH level. But TSH is just one of many thyroid markers. Just because TSH is “normal” does not mean your thyroid is normal. This is why many women get under-diagnosed for hypothyroidism and suffer for years with symptoms that significantly interfere with their health and quality of life.
I am going to walk you through ten lab tests to ask your doctor to run if you suspect you may be suffering from Hashimoto’s. I will explain why to run the test, the typical lab range for results, as well as the optimal range.
TSH
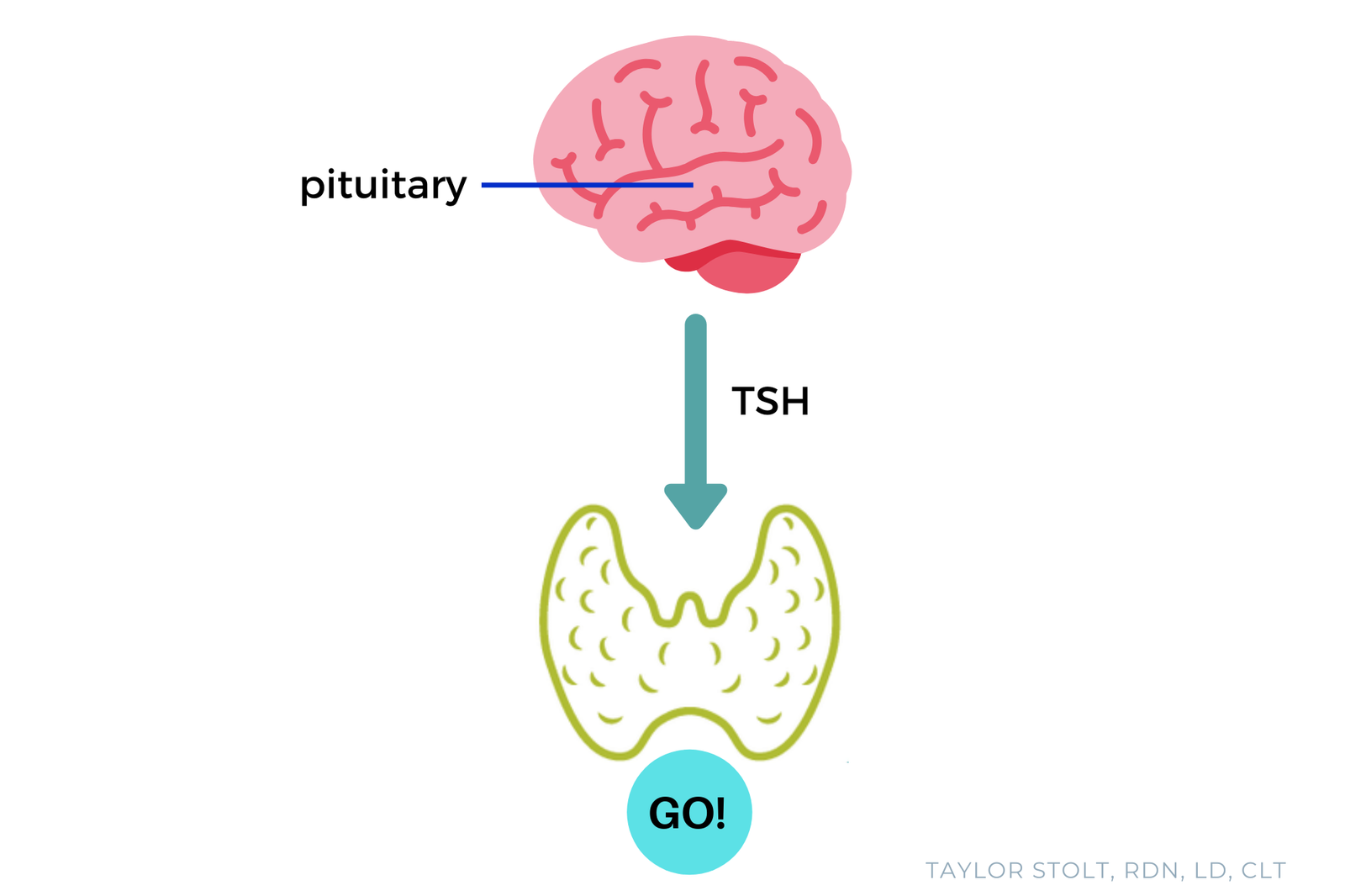
- A specific part of your brain called the pituitary gland produces TSH (thyroid stimulating hormone). It does exactly what it says – stimulates the thyroid. It tells the thyroid to pump out thyroid hormones, both T4 (thyroxine) and T3 (triiodothyroxine).
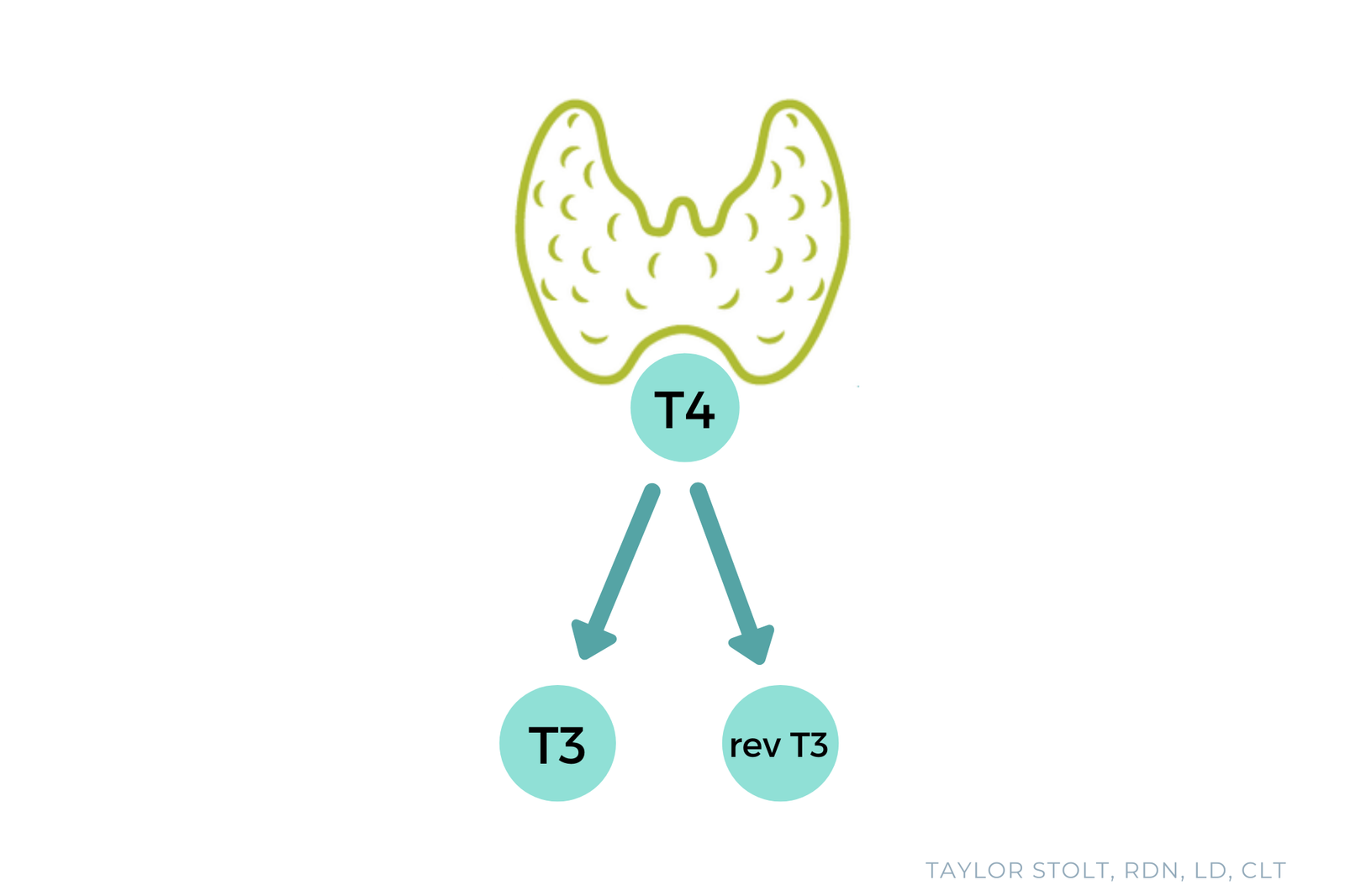
- The problem with running only a TSH level is things could be wrong down-stream. You could have poor production of both T4 and T3, poor conversion of T4 to T3, high reverse T3, or an active autoimmune attack against the thyroid. (Don’t worry, we will cover all of that in detail throughout the rest of this blog post)
- The normal range for TSH varies depending on the lab, but the conventional range is typically 0.5 4-5 mU/L. The National Academy of Clinical Biochemists indicates that 95% of individuals without thyroid disease have TSH concentrations below 2.5 μIU/mL. Most functional medicine practitioners agree that TSH should be 1-2 μIU/mL. In my experience, most of my clients feel best when their TSH is between 1.0 and 2.0.
Lab range: 0.5-5 μIU/mL
Optimal range: 1.0-2.0 μIU/mL
Free T4 and Free T3
- TSH stimulates your thyroid to produce both T4 and T3 hormones, but these thyroid hormones are initially bound up and unable for your body to use.
- Almost 99% of the thyroid hormones in your body are bound to a protein. Protein-bound hormones are large in size so they are unable to bind to receptor sites.
- Thyroid hormones are “metabolically active” after they lose their protein and become “free”. The smaller, “free” thyroid hormones circulate in the bloodstream anywhere from 15 minutes to several hours until they are able to bind to a thyroid receptor site. Thyroid hormones have an effect on the body when and only when they bindto a binding site.
- Both free T4 and T3 perform functions in the body, so it is important to have sufficient levels of both. Free T3 is the most “metabolically active”, meaning it has the biggest impact on how you feel. If TSH and free T4 are normal but free T3 is low, you are likely to experience symptoms of low thyroid function.
- 93% of the thyroid hormones produced are T4, while only 7% are T3. If free T4 levels are normal but free T3 levels are low, this may mean your body is having trouble converting free T4 to free T3. Two nutrients that assist in the conversion of free T4 to free T3 are zinc and selenium.
Lab free T4 range: 0.7-1.53 mg/dL
Optimal free T4 range: 1.0-1.5 mg/dL
Lab free T3 range: 2.3-4.2 pg/mL
Optimal free T3 range: 3.0-4.0 pg/mL
Reverse T3
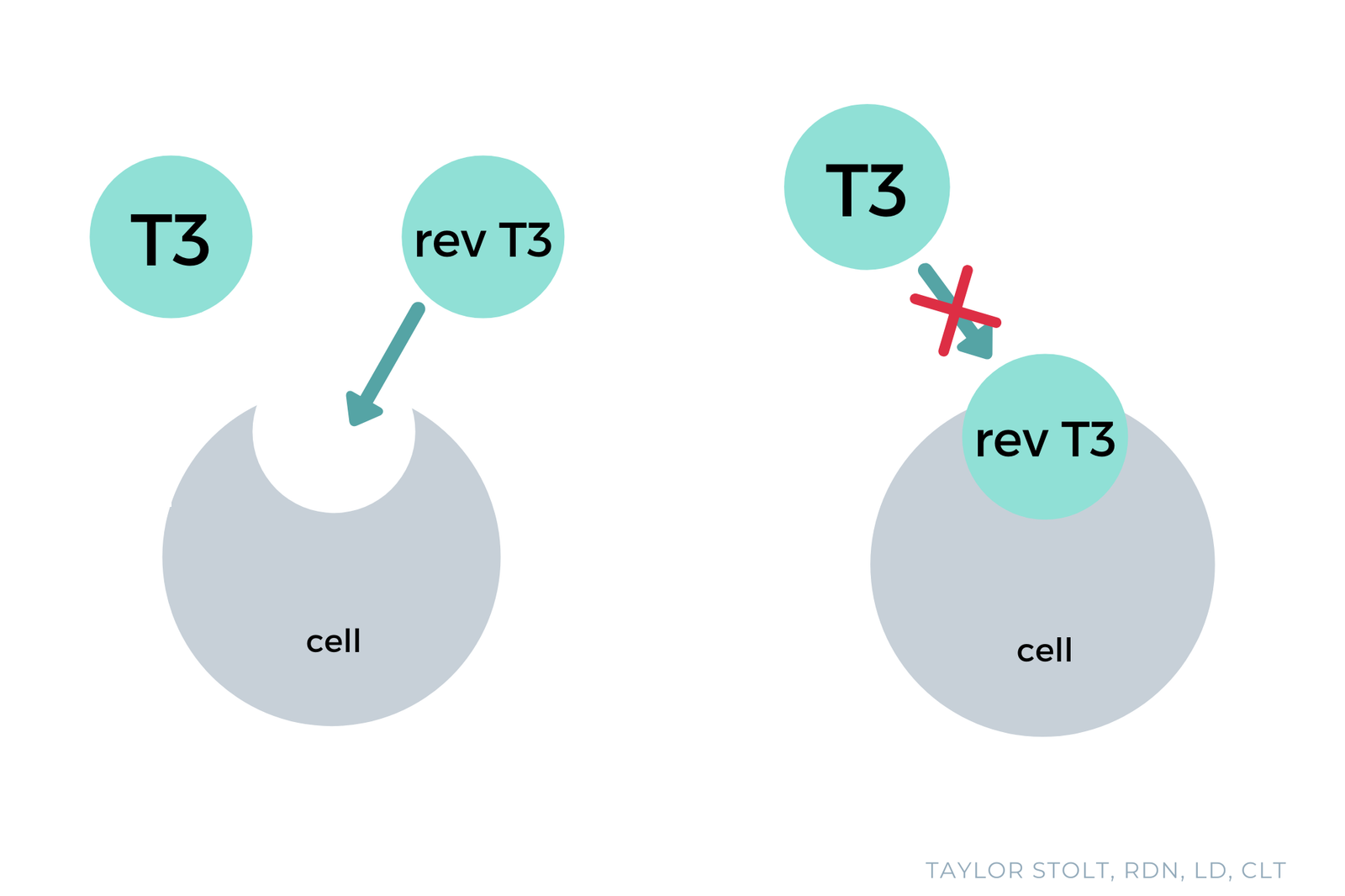
- Reverse T3 is an inactive thyroid hormone. It can bind to the same receptor sites as the active free T3 hormone so if your free T3 looks great but your reverse T3 is high, you have a problem. All of that reverse T3 is blocking free T3 from binding and doing the functions of the thyroid.
- Reverse T3 is produced in response to stress – this could be emotional/mental stress or physical stress due to lack of sleep, a recent surgery, recent pregnancy, undereating, inflammation, toxins, infections. Some medications, such as anti-arrhythmia drugs, heartburn medications and beta-blockers, can also increase reverse T3. Two research studies also showed that iron deficiency may increase reverse T3.
Lab range: 9.2-24.1 mg/dL
Optimal range: 9-18 mg/dL
TPO Antibodies and TG Antibodies
- Thyroid peroxidase (TPO) antibodies are the most commonly elevated antibodies in autoimmune thyroid disease. They are elevated in 90-95% of people with Hashimoto’s. These antibodies are directly responsible for destruction of thyroid tissue.
- Thyroglobulin (TG) antibodies are less likely to be elevated compared to TPO antibodies, but they are still fairly common. TG antibodies are elevated in 60-80% of people with Hashimoto’s.
- Thryoid-Stimulating Hormone Receptor (TSH-R) antibody, also known as thyroid stimulating immunoglobulin (TSI) antibody, is an antibody that indicates Graves disease. If you are experiencing hyperthyroid symptoms make sure you get this marker tested in addition to TPO and TG antibodies. In Graves disease, all three antibodies are typically elevated.
TPO Ab lab range: 0-34 IU/mL
TPO Ab optimal range: 0-15 IU/mL
TG Ab lab range: 0.0-0.9 IU/mL
TG Ab optimal range: 0.0-0.9 IU/mL
Homocysteine
- Homocysteine is an indicator of vitamin B12, B6 and folate status in the body. Serum B12 and folate alone are not good indicators of B vitamin status. Serum B12 and folate only tell you how much is floating around in your bloodstream at the time of the blood draw, not what is actually being utilized by the body.
- Low stomach acid is common in people with Hashimoto’s, which increases the risk for vitamin B12 deficiency. Stomach acid separates vitamin B12 from food proteins, then B12 is able to combine with a protein called intrinsic factor so that B12 can be absorbed and used. Symptoms of low stomach acid include gas, bloating, heartburn, reflux, and a heavy feeling in the stomach after meals.
- Many people with Hashimoto’s have an MTHFR gene mutation. The gene mutation makes it difficult to methylate and activate B vitamins, so your B vitamin status could be low even if you are eating foods that are rich in B12, B6 and folate or you are taking a B vitamin supplement. MTHFR gene mutations can be seen in the raw data “23 and Me” genetic testing – you will just need to find a functional medicine practitioner that can upload the raw data to the appropriate program to generate a user-friendly report.
- Low B vitamin status can contribute to fatigue, weakness, numbness/tingling, brain fog, and difficulty balancing. Elevated homocysteine levels are linked to increased risk of heart disease, dementia, and neurodegenerative diseases.
Lab range: 0-16 µmol/L
Optimal range: 5-7 µmol/L
Vitamin D
- Vitamin D deficiency is a huge problem in the United States. We aren’t getting enough sun exposure and when we do get sun we are slathering sunscreen on, which blocks UVB light and inhibits our body’s ability to make vitamin D from the sun.
- We have decreased our intake of vitamin D-rich foods – liver, organ meats, some seafood, butter and egg yolks. Gut inflammation, adrenal stress, and obesity also increase the risk of vitamin D deficiency.
- Vitamin D deficiency is more common in people with Hashimoto’s. Research shows that more than 90% of people with autoimmune thyroid disease have a genetic defect that decreases their ability to process vitamin D.
- Vitamin D supports T-regulatory cells, which work to keep the immune system balanced and prevent autoimmune disease.
- Research shows that vitamin D supplementation in people with Hashimoto’s that are vitamin D deficient decreases thyroid antibodies.
Lab range: 30-100 ng/mL
Optimal range: 70-100 ng/mL

CRP
- C-reactive protein (CRP) is a marker of systemic inflammation.
- Inflammation plays a huge role in all disease, including Hashimoto’s and other thyroid conditions. High CRP levels are common in people with Hashimoto’s.
- Some research also suggests Hashimoto’s can cause increased inflammation, resulting in increased CRP levels.
Lab range: 0-3 mg/L
Optimal range: <1 mg/L
Ferritin
- Serum iron only accounts for 1% of iron stores in the body while ferritin accounts for over 30%, making it a much better indicator of iron status.
- Low stomach acid production is common in Hashimoto’s, which decreases the body’s ability to absorb iron as well as other minerals.
- Low iron status can contribute to symptoms of fatigue, weakness, pale skin, cold hands/feet, hair loss, headache, chest pain, dizziness, and shortness of breath.
Lab range: 15-150 ng/mL
Optimal range: 70-100 ng/mL
Where to Go From Here
Whether you have been diagnosed with Hashimoto’s or not, if you are suffering from hypo- or hyper-thyroid symptoms I highly recommend scheduling an appointment with your doctor to discuss ordering these labs if they have not been run already. Have an honest, respectful conversation about your symptoms and concerns and be firm when advocating for yourself. I know it can be uncomfortable and scary, but improving your health is well worth it!
If you feel like your doctor is not listening or they refuse to run these tests, you may want to consider another provider. Find a good functional medicine practitioner that is familiar with Hashimoto’s that will take the time to listen and help you explore your health concerns.
Resources
https://www.niehs.nih.gov/health/topics/conditions/autoimmune/index.cfm
https://ghr.nlm.nih.gov/condition/hashimoto-thyroiditis
https://www.ncbi.nlm.nih.gov/books/NBK459262/
https://www.ncbi.nlm.nih.gov/pubmed/7340700
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5422478/#!po=4.72973
https://www.ncbi.nlm.nih.gov/pubmed/12073143